
What is Dry Needling

Trigger Points and Myofascial Pain
So now that we better understand pain, let’s explore dry needling in the management of pain. Specifically pain that comes from the musculoskeletal system. All that means is that the pain is coming from the muscles, joints, fascia, tendons, ligaments, etc. Rather than pain from somewhere else in the body… like an organ (for example, chest pain when having a heart attack, stomach pain when having diarrhea).
To get more specific, we are talking about pain coming just from the muscles or fascia (the connective tissue that lines muscles). This pain is called… myofascial pain! Crazy right…
Pain in muscles or fascia comes from trigger points. Myofascial trigger points are defined as “highly localized, hyperirritable spot in a palpable, taut band of skeletal muscle fibers.” All this means is that a trigger point is a knot in the muscle that you can actually feel and that it is painful. You probably can find a few of these knots on your body right now. Especially around the neck and shoulders if you do a lot of work on the computer!
Trigger points also have other unique qualities. They can create referred pain, meaning they trigger pain elsewhere (the pain refers to other areas than just the location of the knot). And they create local twitch responses, meaning the knots will spasm when you apply pressure to them.
According to this clinical review, myofascial trigger points were the primary source of pain in 30-85% of patients with pain who went to a primary care setting, pain clinic, neurologist, dental clinic, internal medicine practice. However, it often goes undiagnosed leading to chronic conditions. Although no single treatment strategy has proved to be universally successful, dry needling has evidence that supports its effectiveness in management of this type of pain!
“Dry needling is a skilled technique performed by a physical therapist using filiform needles to penetrate the skin and/or underlying tissues to affect change in body structures and functions for the evaluation and management of neuromusculoskeletal conditions, pain, movement impairments, and disability.” –Federation of State Boards of Physical Therapy
Physical therapists, like myself, use a very thin small needle (called a filiform needle) that does not inject any fluid into the body. That’s why it is called “dry” needling. These needles are very similar to acupuncture needles, but dry needling is different from acupuncture. To understand the difference, we must dive a little deeper into the common conceptual models of dry needling… what is actually happening when we put this tiny needle into the knot in the muscle? And how does that get rid of pain?
Common Conceptual Models of Dry Needling
The basics start with two common conceptual models.
The first is the Radiculopathy model, described by Dr. Gunn. Dry needling is used to stimulate inside of the muscle, it is an “intramuscular stimulation technique.” The premise is that myofascial pain syndrome is the result of peripheral neuropathy or radiculopathy. Meaning there is a change in the nerves that supply the muscle, either inside of the actual muscle or around the start of the nerve in the spinal cord. This change, called “denervation” means there is a restricted flow of nerve impulses. And this denervated tissue becomes super sensitive. In muscles, this leads to muscle shortening, pain, and trigger points.
This supersensitivity can occur within the actual muscle where the knot is, or it can occur along the paraspinal muscles that support the spine. The paraspinal muscles (also called erector spinae muscles) run along the vertebra, right next to the nerve roots coming out of the spinal cord. Muscle shortening in the paraspinals puts pressure on the nerve root, which restricts the flow of nerve impulses to all innervated structures resulting in atrophy, irritability, and sensitivity.
The second model we will take a closer look at is the Myofascial Trigger Point Approach, described by Travell and Lewit.
Dr. Janet Travell was JFK’s personal physician. She’s a pretty amazing women in medicine, and her work on this topic is probably the most comprehensive to date. I could go on a very long winded tangent about her and her work, but let’s stick to how her model describes dry needling as a treatment for myofascial pain.
Microscopic changes are occurring in the muscle fibers within the trigger point. When a muscle is overloaded or incorrectly loaded, oxygen and other nutrients are depleted from the muscle and the fibers become stuck in a contracted state. They are shortened and unable to relax.
First done with injections, Travell realized the effect was primarily due to the mechanical stimulation with the needle, rather than due to what “wet” fluid was injected. The dry needle creates a “local twitch” which is a rapid depolarization of the involved muscle fibers. After twitching, the spontaneous electrical activity in the muscle subsides and pain and dysfunction decreases dramatically.
Effectiveness of Dry Needling
The effectiveness of dry needling has been evaluated in numerous randomized control trials, and several comprehensive systematic reviews. Systematic reviews are the highest level of evidence, where all the available evidence from individual randomized control trials are brought together to present an overall effectiveness of the intervention.
These systematic reviews show evidence that dry needling is an effective treatment for myofascial pain. I’ve highlighted a few of them below, and you can find reference links at the end so that you can do more of your own research!
- In a 2001 systematic review, 23 randomized controlled trials were included in which some form of needling (dry needling or injections) was used to treat myofascial pain. The conclusions shows that direct needling of trigger points appears to be an effective treatment, and that the effect is likely due to the needle or placebo rather than the “wet” injection.
- The 2005 results of a Cochrane systematic review of 35 randomized control trials indicated that dry needling for low back pain has evidence for short term pain relief and function improvement compared with no treatment or sham therapy.
- From the 2013 Journal of Orthopaedic & Sports Physical Therapy, dry needling was recommended, compared to sham or placebo, for decreasing pain immediately after treatment and at 4 weeks in patients with upper-quarter myofascial pain syndrome.
- In 2015, Liu et al concluded that TrP dry needling can be recommended for the treatment of neck/shoulder pain at the short term and midterm follow-up assessments
- Just recently, in February 2021, a new systematic review and meta-analysis was published in the Physical Therapy & Rehabilitation Journal. There is moderate- to low-quality evidence that suggests positive effects of trigger point dry needling for pain intensity and pain-related disability in nontraumatic shoulder pain.
I may have gotten a little side tracked with my literature review… What it boils down to is that there IS evidence out there that supports dry needling for treating pain. Unfortunately, further research is still needed. May issues arise in the ability to assess the effectiveness of dry needling, and with as new as this field is, there just hasn’t been enough time to evaluate all of the intricacies of this practice. It was just in 1983 that Travell and Dr. David Simons published their work, called “Myofascial Pain and Dysfunction – The Trigger Point Manual.”
But the current results are promising! And personally, I can attest to the effectiveness of this method in my practice every day as a physical therapist. With the opioid crisis still raging on, and many individuals struggling to manage their pain without the use of medications or surgery, we must continue to expand modern medicine and learn about the effectiveness of alternative treatment options to manage pain.
Where can you get dry needling?
Dry needling is a skilled intervention by physical therapists. You should always seek health care treatment from a licensed professional. Physical therapists are licensed health care professionals and are guided by our education, experience, professional responsibilities and competence, and legally defined scope of practice.
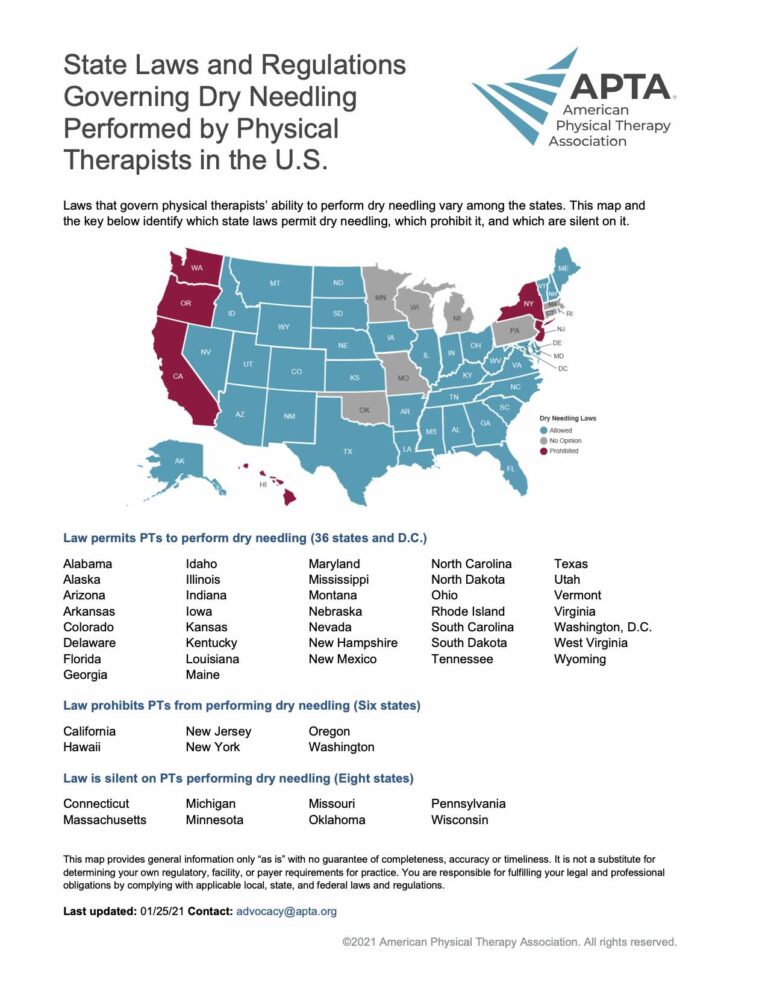
The scope of practice is defined by practice acts. Each state has a specific set of a rules and regulations that define whether or not a specific procedure, technique, or modality falls within that scope of practice. In 36 states and D.C. the law permits physical therapists to perform dry needling. It is prohibited in 6 states, and the other 8 states are silent on it.
Check out the awesome map by the American Physical Therapy Association to see if your state allows dry needling.
If your state does allow dry needling by physical therapists, you should still ask your physical therapist questions regarding their training in dry needling to ensure their competency with this technique.
I was fortunate enough to be initially trained in trigger point dry needling within my doctorate physical therapy program. I then acted as a teaching assistant for the course the following year and assisted in the training and assessment of basic dry needling ability of other physical therapy students. I have practiced dry needling in the clinical setting for 8 years. During that time, I have also completed 3 advanced level continuing education course programs through Myopain Seminars amounting to an additional 100 contact hours in the theory, practice and clinical application of dry needling. In 2023, I passed practical and theoretical examinations to achieve my certification as a Certified Myofascial Trigger Point Therapist specializing in Dry Needling, CMTPT/DN.
As you can tell, I am very passionate about this technique and in continuing to expand my knowledge and skill to better serve my patients and clients on their healing journey. I use this technique daily and I see excellent results!
References
Kalichman L, Vulfsons S. Dry needling in the management of musculoskeletal pain. The Journal of the American Board of Family Medicine. 2010 Sep 1;23(5):640-6.
Systematic reviews:
Cummings TM, White AR. Needling therapies in the management of myofascial trigger point pain: a systematic review. Arch Phys Med Rehabil 2001;82: 986 –92.
Furlan AD, van Tulder MW, et al. Acupuncture and dry-needling for low back pain. Cochrane Database Syst Rev 2005;(1):CD001351.
Kietrys DM, Palombaro KM, Azzaretto E, Hubler R, Schaller B, Schlussel JM, Tucker M. Effectiveness of dry needling for upper-quarter myofascial pain: a systematic review and meta-analysis. journal of orthopaedic & sports physical therapy. 2013 Sep;43(9):620-34.
Liu L, Huang Q-M, Liu Q-G, et al. Effectiveness of dry needling for myofascial trigger points associated with neck and shoulder pain: a systematic review and meta-analysis. Arch Phys Med Rehabil. 2015;96:944–955.
Navarro-Santana MJ, Gómez-Chiguano GF, Cleland JA, Arias-Buría JL, Fernández-de-Las-Peñas C, Plaza-Manzano G. Effects of Trigger Point Dry Needling for Nontraumatic Shoulder Pain of Musculoskeletal Origin: A Systematic Review and Meta-Analysis. Phys Ther. 2021 Feb 4;101(2)